


Treatment of pediatric soft tissue wounds presents additional complexities and highlights unique requirements. This piece provides a synopsis of an article [1] published in the Journal of Pediatric Surgery Case Reports by Dr. Kyle Crowley and his colleagues from the Division of Paediatric Surgery at Townsville University Hospital in Queensland, Australia.
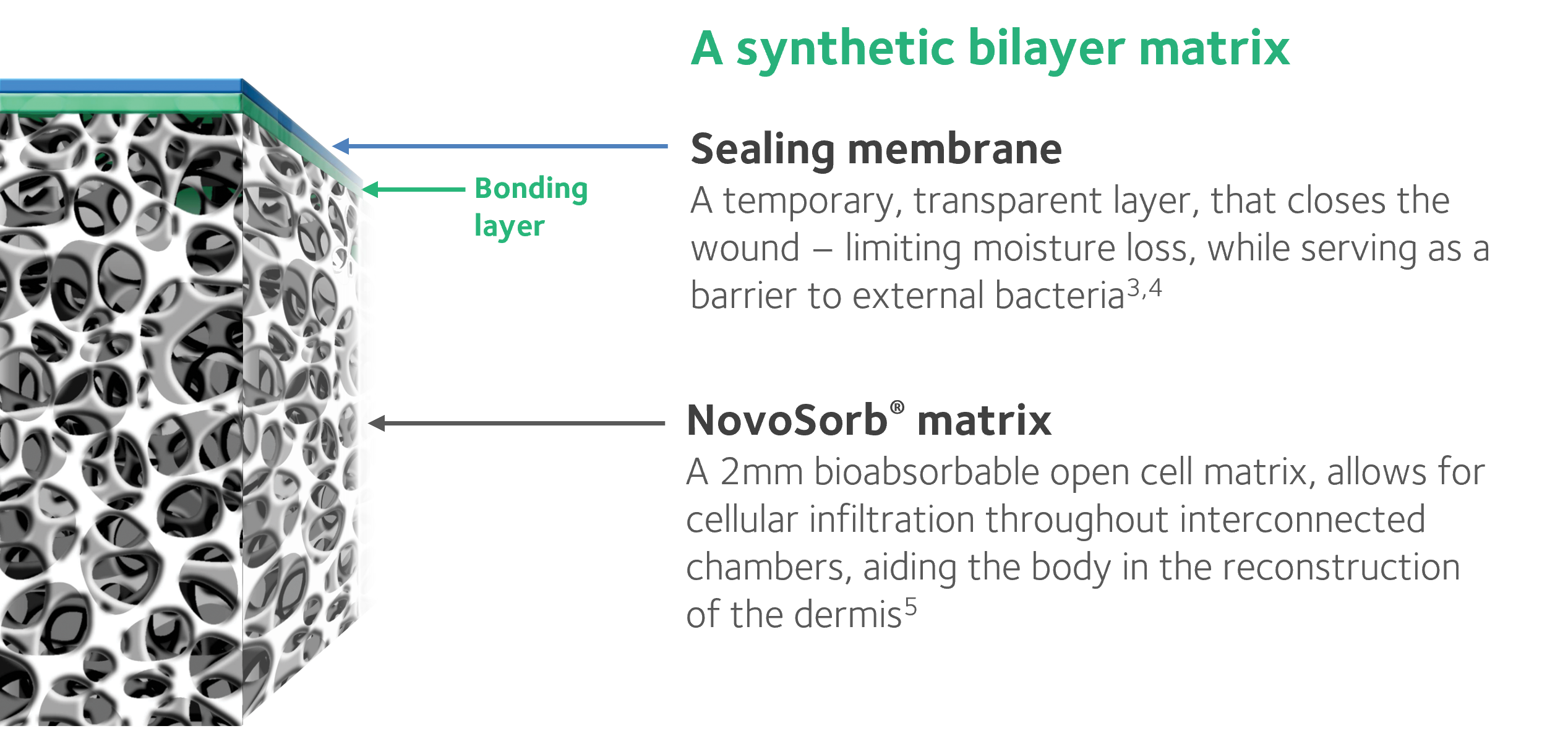
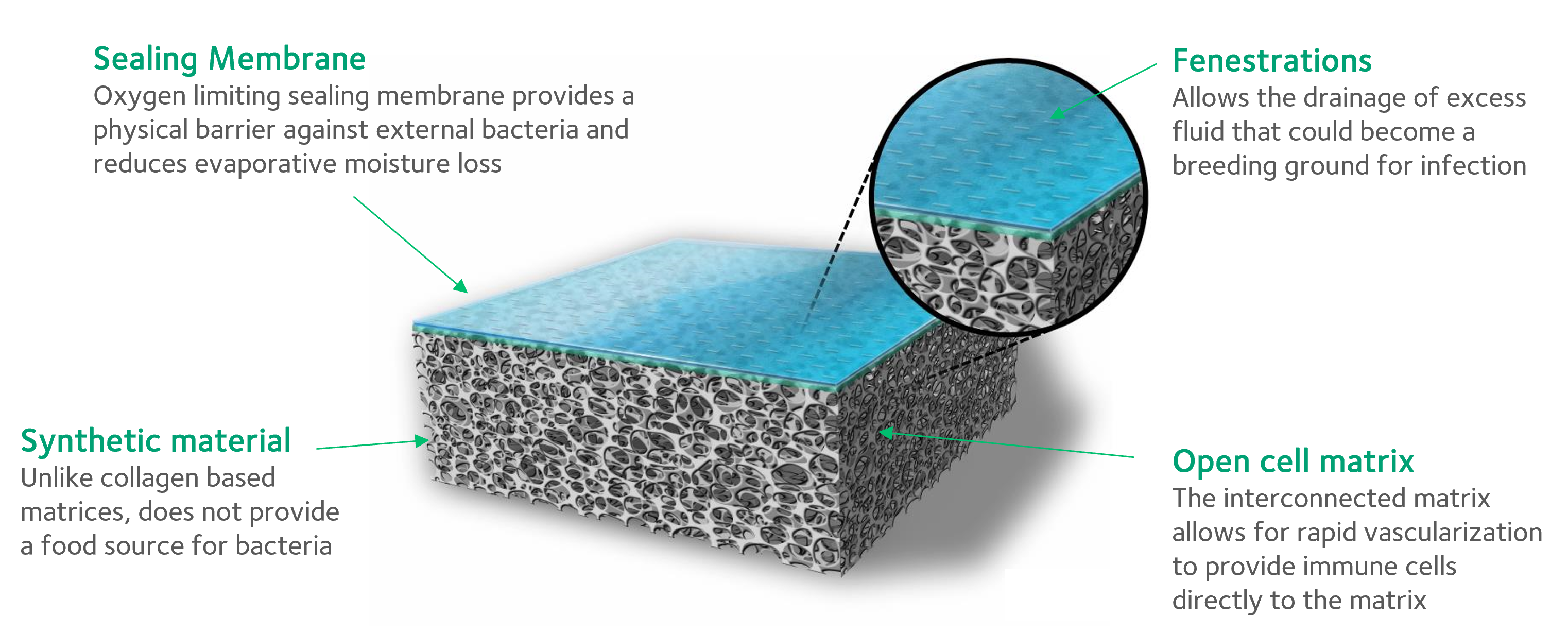
NovoSorb® BTM, a biodegradable temporizing matrix (i.e., dermal scaffold), was applied in a two-stage repair to temporize the patient’s wounds and aid in generating new dermal tissue. This case illustrated the need for a dermal substitute that delivers long-term clinical outcomes supportive of pediatric needs.
The authors present a case report of a 9-year-old boy who was involved in a traumatic incident in which he was dragged underneath a vehicle, resulting in traumatic abrasions over approximately 25% of his total body surface area (TBSA), affecting his groin, left and right thighs, and lower abdomen. The patient also suffered a degloving injury to his penis, a left iliac crest fracture, and avulsion injuries to the scrotum and bilateral testicles.
The repair of extensive skin and soft tissue injuries in children can be challenging due to large areas of soft tissue loss and limited reconstructive options. Variables under consideration for procedure selection are as follows:
– This child resided in a remote location post-discharge and would potentially have limited opportunities for routine monitoring compared to an urban setting [2]—the procedure needed to ensure the best chance of a successful outcome at first surgery.
– The patient was presented with an absence of epidermal potential and poor dermal structure, including good support for skin grafts. A dermal substitute offered benefits in this case.
– The nature of the injury (traumatic abrasion from the road) caused concern for maintaining a healthy wound bed. BTM offered the advantages of being clinically shown to be robust in the presence of infection. [3]
Surgical Techniques Used to Repair Deep Soft Tissue Injuries
The patient underwent a two-stage repair of the injuries with the application of NovoSorb BTM, a fully synthetic bilayer open cell matrix. Staged reconstruction of the child’s deep soft tissue deficits was performed in which a split skin graft followed BTM application. The surgical team used the following procedures to repair the child’s injuries:
– Contaminated wounds were immediately washed and dressed in a silver sulfate-foam bandage and synthetic adhesive.
– On day 5, following further wound washout and debridement, BTM was applied to the patient’s lower abdomen, left hip, right thigh, left suprapatellar region, and scrotum. BTM was secured using staples and dressed in a silver sulfate-foam bandage, followed by the application of a vacuum-assisted closure (VAC) dressing to manage fluid exudate over the large wounds. Splints were used to prevent any shearing motion and to give BTM the best chance of integration.
– The VAC dressing was checked and changed on operating theatre days 3, 6, and 10 post- BTM application. VAC dressing was discontinued on day 22 post-BTM application due to fecal and urine soiling and difficulties achieving a good seal. Standard dressing changes continued.
– On day 34 post-application, BTM was assessed as fully integrated.
– On day 36, BTM was delaminated, the wound bed was prepared for the placement of grafts, and the patient underwent meshed split-thickness skin grafting, which was secured using staples and dressed in a nonadherent silicone wound contact layer, silver sulfate-foam bandage, perforated plastic film, and synthetic adhesive.
– On day 12 post-grafting, all dressings and staples were removed. Intensive rehabilitation commenced.
Clinical Outcomes Achieved Using NovoSorb BTM
The patient remained hospitalized for two months to allow the BTM to fully integrate and the skin graft to heal. Despite the lengthier hospital stay required, the surgeons concluded the additional time was worthwhile due to the good early clinical outcomes achieved in terms of cosmesis and skin suppleness at the time of the patient’s discharge 21 days after skin grafting, which would have been difficult to achieve using thin meshed grafts alone.
The authors also reported 100% take of the skin grafts over the integrated BTM, achieving durable wound coverage with minimal wound contraction after skin grafting and a low incidence of complications such as infection.
Improving Outcomes, Changing Lives
In this case, BTM has demonstrated the successful management of deep soft tissue injuries in a pediatric population. To view further literature supporting the use of BTM in a pediatric population, visit our website or contact one of our knowledgeable team members at (302) 268-6163.
References:
[1] Crowley K, Balaji S, Stalewski H, Carroll D, Mariyappa-Rathnamma B. Use of Biodegradable Temporizing Matrix (BTM) in large trauma-induced soft tissue injury: A two-stage repair. Journal of Pediatric Surgery Case Reports. 2020; 63:101652.
[2] Personal communication with the author.
[3] Greenwood JE, Dearman BL. Comparison of a sealed, polymer foam biodegradable temporizing matrix against Integra® dermal regeneration template in a porcine wound model. Journal of Burn Care & Research. 2012; 33(1):163-73.
[4] Dearman BL, Li A, Greenwood JE. Optimization of a polyurethane dermal matrix and experience with a polymer-based cultured composite skin. Journal of Burn Care & Research. 2014; 35(5): 437-48.
[5] Wagstaff MJD, Schmitt B, Caplash Y, Greenwood JE. Free flap donor site reconstruction: A prospective case series using an optimized polyurethane temporizing matrix. Eplasty. 2015; 15:231–48.